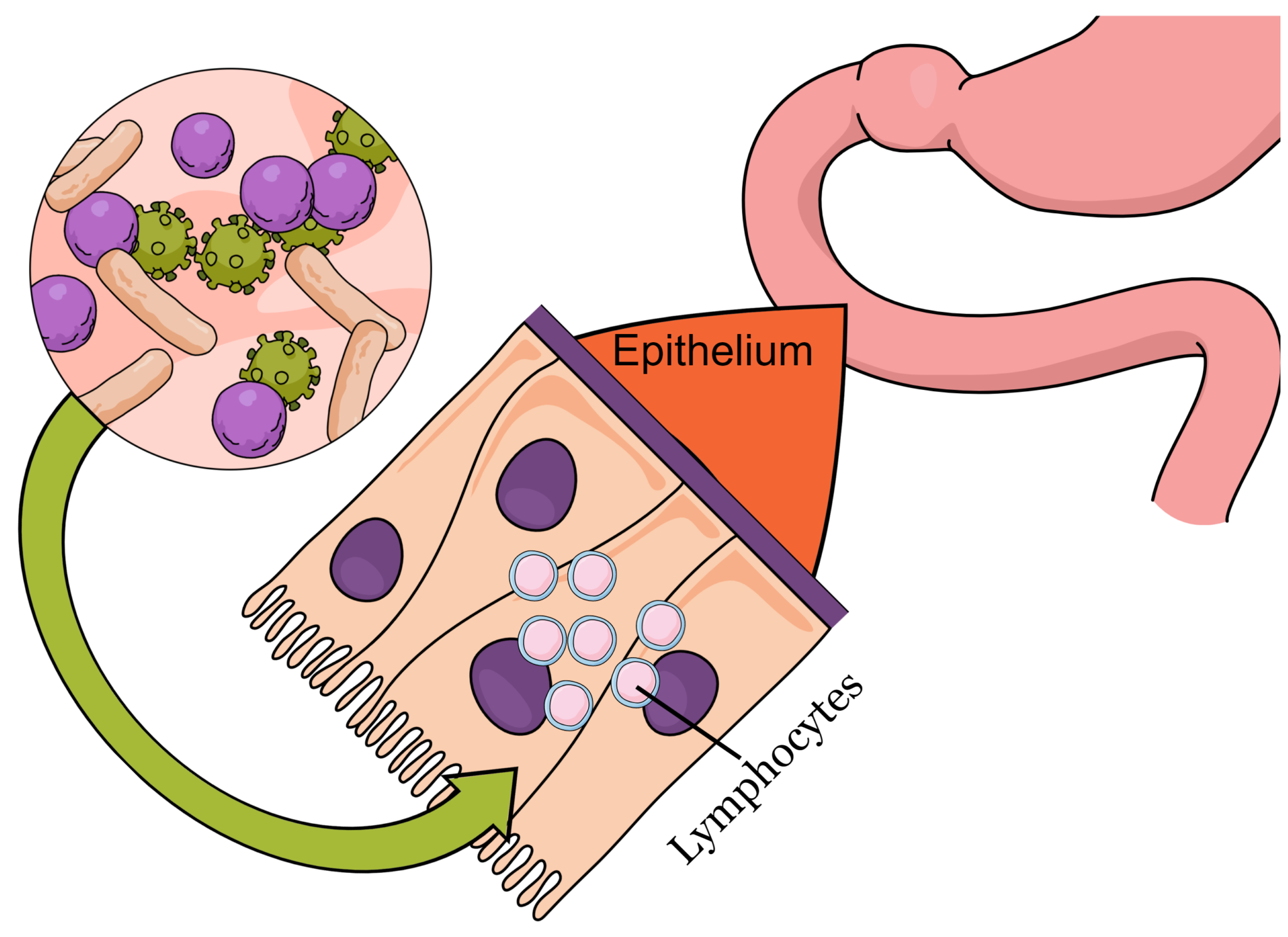
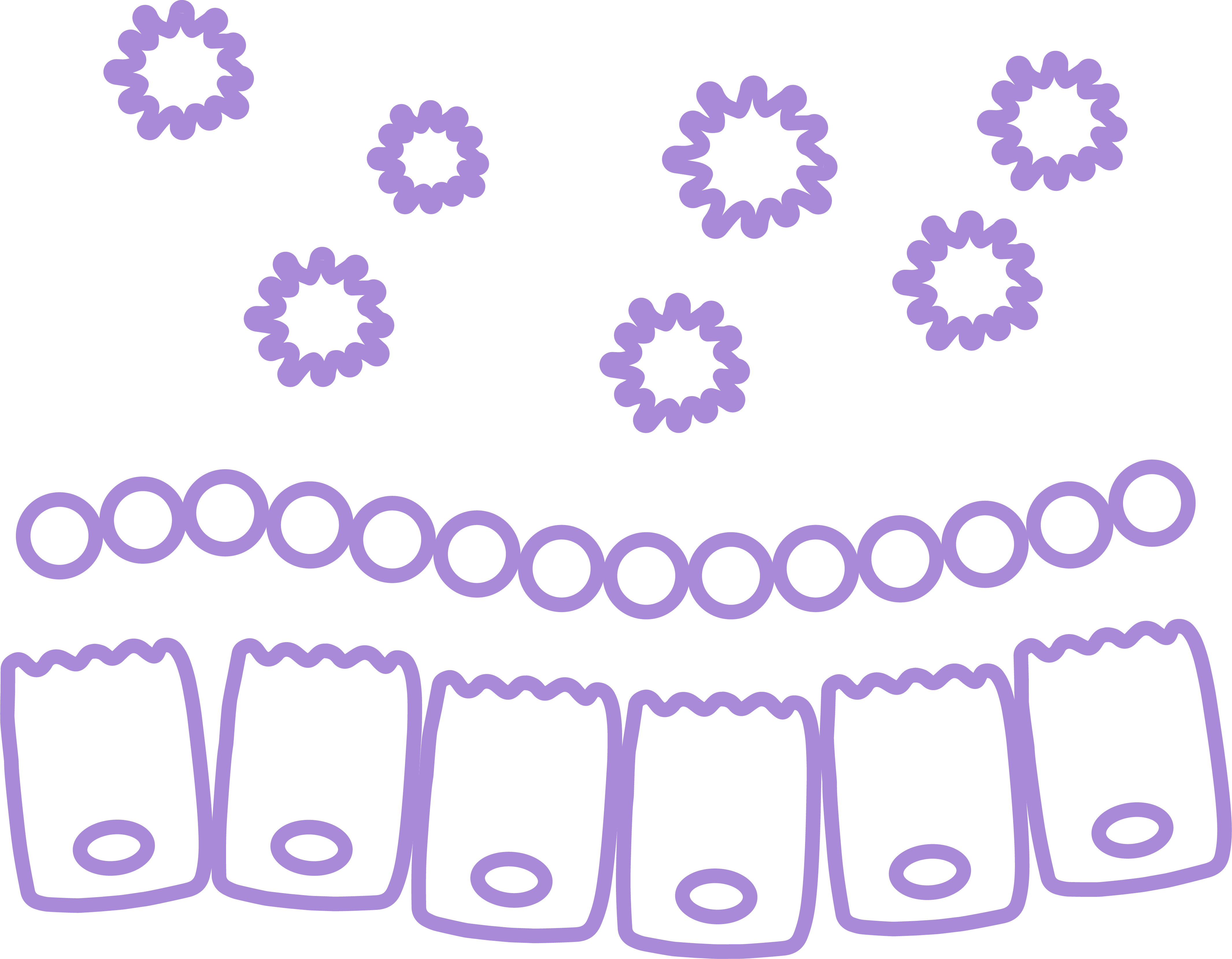
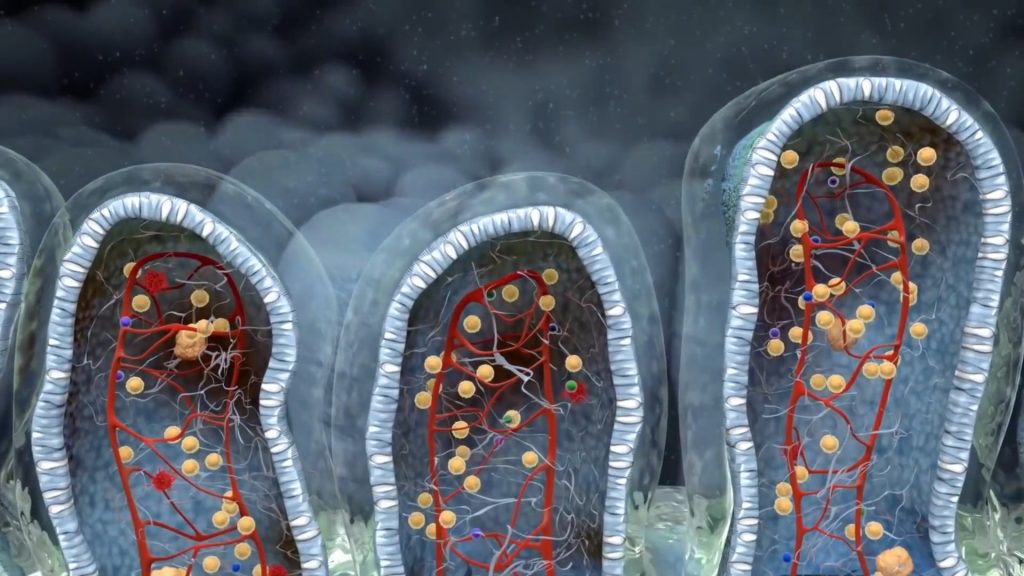
The hallmark of celiac disease is lymphocyte infiltration in the epithelium. This produces villus atrophy which may be seen nad measured with a simple endoscopy. The symptoms of celiac disease are attributed to this exact infiltration. Nevertheless, the same lymphocyte infiltration may manifest due to other reasons, most notably chronic infections and microbial overgrowth. In fact, even commensal bacterial overgrowth may lead to loss of immune tolerance and mimic the exact mechanism that celiac disease exploits to produce symptoms.
Bacterial overgrowth may produce intraepithelial lymphocyte infiltration and mild villous atrophy, mimicking celiac disease
Nick is a 26 y.o marketing advisor. He was born via c-section as was his younger brother. When his was 5 years old he had his appendix and tonsils removed within a period of 7 months. His mother reports that ever since he had been suffering from at least one severe infection (either gastroenteritis, or bronchitis) every year and had to take at least one antibiotic treatment per year. 3 years ago his gastrointestinal symptoms appeared after consuming a large amount of seafood. The next morning he woke up with very upset stomach and only calmed down after vomiting 5 times. He remembers that from that point and on he would experience at least one diarrhea per week and he could not tolerate wheat containing foods. 6 months later he had lost 11 kg and bloating/gas was a daily phenomenon.
He has visited several specialties so far. He has performed 2 colonoscopies and 2 gastroscopies. His blood work and the duodenal biopsies are indicative of celiac disease. This is why he has been on a strict gluten free diet for the past 2,5 years. Nevertheless, he has only slight improvement, the diarrheas have not stopped and he has only gained back 2 kg. He also got the diagnosis of Hashimoto’s thyroiditis two years ago. The only period he felt better was a 2-month interval after rifaximine.
Trigger - Effect timeline
Tonsillectomy/ Appendectomy
Reduced sIgA produvtion
All day eater
MMC inhibition
Antibiotics
Microflora diversity diminishing
Extreme SIBO
Intraepithelial infiltration
IBSyncrasy
not every ibs is the same. find yours! over 1400 real cases.
Diarrhea may result from chronic small intestinal bacterial overgrowth
Weight loss
Small intestinal bacterial overgrowth hinders proper luminal preparation of food. Indigested particles cannot be efficiently absorbed.
Frequent infections
Bacterial overgrowth conditions the colonic and intestinal environment making it prone to pathogenic bacterial colonization and infection
Bloating/gas
Excessive gas production is attributed to extensive and potent fermentation of starch and fiber early in digestion
USEFUL DATA MINED
Absence of HLA DQ2/8
Antibiotic abuse
Partial villus atrophy
Intraepithelial lymphocytes
Marginally elevated tTG antibodies
All day eater
Tosnillectomy/appendicectomy
Hashimoto's thyroiditis
Results
Nick was the patient with the highest SIBO breath test values I had seen. sIgA deficiency was prominent, probably aggravated by early appendix and tonsils removal. In addition, his all-day eating habits fed constantly his small intestinal bacteria never leaving time for Migration Motor Complex to clean the area. Serum IgA deficiency could also explain the recurrent infections and the tons of antibiotics he had consumed.
Actionable exam results
Pseudomonas aeruginosa
A duodenal pathogen with characteristic gluten elastase activity. Pets suffering from otitis are common carriers of this bacterium
sIgA deficiency
Potent predisposition for infections. Reduced mucosal immunity
SIBO
Extreme fermentation of sugars and starch, diminished absorption and augmented leaky gut
Probiotic sterility
Not a sign of Lactobaciili or Bifidobacteria on stool due to antibiotic abuse
Treatment
The recession that Nick entered after taking rifaximine was not accidental. The values recovered from his SIBO test were very high. The proposed treatment in this case is three 10-day sequential treatments with rifaximin over 3 months. At the same time, an attempt should be made to increase secretory immunoglobulin A. Butyrate, S. bulardii, beta glucans, must be included, whereas recolonization of certain beneficial populations, such as Lactobacilli is also very important. Common probiotics are usually of no benefit, and in fact may even worsen the symptoms adding to the overgrowth. In addition, dietary and behavioral changes are of great importance as they allow for faster recovery.
Follow up
The schedule Nick was given was 90-day long and extremely strict. But he did manage to follow it. It is very important to stick to the dietary and behavioral interventions as this kind of IBS has its roots early in the small intestine and thus it is very easy for the symptoms to bounce back.
Bullets
Celiac disease is not the only cause of intraepithelial lymphocytes observed in duodenal biopsies
SIBO, NSAID use and viral infections may produce celiac disease-like image
Single rifaximine treatment usually is not enough when SIBO is that extended
Vitamin and other nutrient deficiencies are very common and should be addressed immediately
Choices in lifestyle and diet play a decisive role in the way in which bacterial overgrowth will manifest
Theodoros Prevedoros, MSc
The Microbiome Biochemist
With extensive experience evaluating over 3000 cases in various specialties, including gastroenterology, pediatrics, and endocrinology, Theodoros has collaborated with more than 25 doctors from Greece and Cyprus and over 10 laboratories worldwide.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of all the cookies. Accept
Manage consent
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.