Irritable bowel syndrome and anemia
Irritable bowel syndrome and anemia are connected, and IBS increases the risk of iron deficiency and iron deficiency anemia. The link comes from reduced intake during flares, blocked absorption from common foods and medicines, and occasional blood loss or overlapping conditions. In practice, IBS does not usually cause anemia outright, but it does make low iron much more likely
Table of Contents
Irritable bowel syndrome and anemia
IBS is a functional bowel disorder, yet people with IBS often have lower baseline micronutrient levels including iron compared with non-IBS controls, which raises the risk of iron deficiency anemia. A systematic review reported lower vitamin B2, vitamin D, calcium, and iron at baseline in IBS cohorts. Anemia itself is not a typical IBS feature and when iron deficiency anemia is present it is a red flag that needs evaluation for other causes like bleeding or malabsorption. The Merck Manual lists iron deficiency anemia among the red flags that warrant investigation.
IBS subtypes behave differently, and knowing your pattern reduces guesswork. If you are not sure where you fit, start with understanding your specific IBS subtype before changing diet or supplements.
Are IBS and anemia related?
Yes. People with IBS tend to show lower baseline micronutrient levels including iron, and anemia is considered an alarm feature that should trigger a targeted workup for non-IBS causes. In practice, IBS functions as a risk amplifier for low iron rather than a direct cause of anemia. Evidence for the association comes from cohort syntheses showing lower iron status in IBS and from studies where anemia in suspected IBS predicted organic disease rather than IBS itself. See the multicenter study on alarm features and the micronutrient review.
Symptoms of anemia and when people with IBS need a workup
Symptoms of anemia include easy fatigue, shortness of breath on exertion, palpitations, lightheadedness, ice craving, and pale skin. The lab picture usually shows low ferritin and may show microcytosis with low hemoglobin. If you notice black or tarry stool, visible blood, or unexplained weight loss, seek prompt evaluation because these are not IBS symptoms and they raise concern for another cause.
Can irritable bowel syndrome cause iron deficiency?
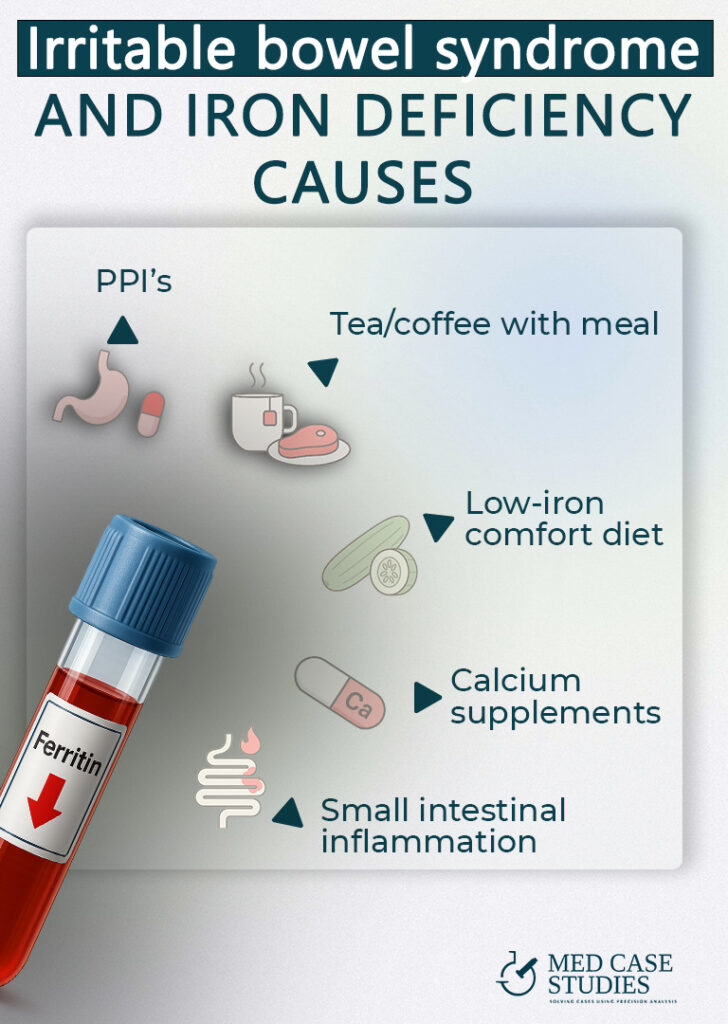
It definetly increases the likelihood of iron deficiency through lower intake during flares and reduced non-heme iron absorption when tea, coffee, calcium, or proton pump inhibitors are used. Restrictive phases such as a strict low FODMAP diet can also reduce micronutrient intake if not supervised. Guidance recommends evaluating iron deficiency anemia for gastrointestinal sources rather than assuming IBS alone. See the AGA workup guidance and classic data on tea and coffee inhibiting absorption and PPIs suppressing non-heme iron.
IBS-predisposed anemia versus iron deficiency anemia from other cause
Think of IBS as a risk amplifier. Food avoidance during flares lowers iron intake. Medications and beverages can block non-heme iron absorption. Separate conditions can cause blood loss that reduces iron stores. That is why checking ferritin and iron studies is important, and why stool testing or endoscopic evaluation may be needed if there are alarm features such as rectal bleeding, black stools, or weight loss.
Why people with IBS may have low iron or iron deficiency
01
Dietary restriction
Lower iron intake during strict low FODMAP or when legumes and red meat are reduced
02
Absorption inhibitors
Coffee and tea polyphenols phytates in grains and legumes and calcium at the same meal
03
PPIs and low acidity
Proton pump inhibitors reduce non heme iron absorption even when intake is adequate
04
Enhancers and timing
Pair iron rich foods with vitamin C and keep coffee tea and calcium away from that meal
Day-to-day choices matter. A low FODMAP phase or other restriction can reduce overall micronutrient intake, including iron, if it is not guided and re-expanded. In a randomized program, the low FODMAP arm had a significant decrease in several micronutrients compared with a standard IBS diet, indicating a real risk if the diet is not supervised.
Iron absorption basics and how to increase iron absorption from food
Non-heme iron from plants depends on the intestinal environment. Vitamin C pairing increases non-heme iron uptake, while polyphenols in tea and coffee, phytates in grains and legumes, and calcium from dairy reduce absorption. Calcium uniquely inhibits both heme and non-heme iron at the point of initial uptake, so timing matters. Practical takeaway: pair iron-rich foods with a vitamin C source and avoid tea, coffee, and calcium around the same meal. Evidence overview in StatPearls.
Low FODMAP diet pitfalls
During the strict low FODMAP phase, people often drop legumes and some grains that carry non-heme iron. If meats are also limited due to symptoms, total iron intake can fall. Data on micronutrient shortfalls during low FODMAP phases come from Eswaran 2020.
PPIs, tea, and calcium can cause digestive problems with iron absorption
Proton pump inhibitors reduce gastric acidity and suppress the absorption of dietary non-heme iron. This has been shown even when intake is adequate. Tea and coffee are potent inhibitors of non-heme iron absorption in humans, which is why beverage timing matters for people with IBS who already struggle with intake. Calcium blocks both heme and non-heme uptake at the enterocyte, so avoid pairing high-calcium foods or supplements with your iron-rich meal. StatPearls. For PPI-focused cases, see my case study on long-term PPI use complicating IBS.
When oral iron supplements trigger digestive problems in IBS
Oral iron commonly causes abdominal pain, bloat, stool darkening, and diarrhea or constipation. Beyond symptoms, luminal iron can shift the gut microbiome toward potentially pro-inflammatory patterns in some settings. A review summarizes that oral iron may adversely affect the intestinal microbiota.
Oral iron may increase Enterobacteriaceae and cause digestive problems
In adults, ferrous bisglycinate increased the relative abundance of Enterobacteriaceae in a controlled study, which aligns with reports that excess luminal iron can favor pathobionts. Clinically, that shift means more gas, urgency, or loose stool for people with IBS who are already sensitive to microbial and metabolic changes.
Diarrhea, bloat, abdominal pain, and stool changes with iron supplement use
Many people with IBS report that standard oral iron worsens diarrhea, bloat, or abdominal pain. If an oral trial is essential, using the lowest effective dose, alternate-day dosing, or slow-release formulations can sometimes improve tolerance, yet symptoms can still persist. After antibiotics, animal data suggest oral iron may hinder microbiota recovery, which is another reason to be cautious soon after antibiotic courses. In our practice we see this pattern often, especially in people with post-infectious IBS or recent antibiotic exposure.
learn how your gut works in real life and find your ibs type and treatment in IBSYNCRASY
-
DIAGNOSIS
TREATMENT
-
FOLLOW UP
My stance on treatment: Avoid oral iron, prefer IV infusion under supervision, liposomal iron supplement only in very extreme cases
Because IBS is a microbiome-sensitive condition, our GI-microbiome–first stance is to avoid oral iron whenever possible, to protect the gut environment and symptoms. We prefer medically supervised intravenous iron when iron repletion is necessary, since it bypasses the intestinal lumen and is effective without exposing the gut to unabsorbed iron. Best-practice advice supports IV iron when oral iron is not tolerated, ineffective, or absorption is compromised. See the AGA 2024 Clinical Practice Update. We reserve liposomal oral iron for very extreme situations where IV is not feasible and a short, closely monitored course is the only practical option.
Why IV iron protects the gut barrier
IV iron achieves repletion quickly without leaving free iron in the intestinal lumen, which reduces the chance of feeding Enterobacteriaceae or aggravating IBS symptoms. It avoids beverage and calcium interactions, and it is not limited by PPI therapy. In our experience with people who have IBS and low iron, symptom stability is often better when IV iron is used under supervision compared with repeated oral trials.
How and when a liposomal iron supplement may be used
I recommend liposomal iron only in rare scenarios when a carefully monitored, short oral course is unavoidable. Even then, we space it away from tea, coffee, and calcium, pair with vitamin C, and stop if abdominal pain, diarrhea, or bloat escalate. If intolerance appears, we stop and route to IV iron rather than forcing adaptation.
Diet and daily habits that help increase iron while also managing IBS
Choose heme iron sources you tolerate and pair non-heme iron with vitamin C. Re-expand a low FODMAP diet to include iron-containing foods as soon as your symptoms allow. If SIBO or another condition is suspected, address it because overlapping issues can lower iron or vitamin B12. Learn why diagnosing the specific bacterium in SIBO can influence iron and B12 status.
Heme and non heme sources of iron and vitamin C pairing to absorb iron
Heme iron from meats is absorbed more efficiently and is less affected by inhibitors. Non-heme iron from legumes, fortified grains, nuts, and leafy greens benefits from vitamin C pairing. Keep a weekly rotation that fits your IBS subtype and symptoms, and avoid combining your iron-rich meal with tea, coffee, or calcium.
The complete end list to boost your iron safely and increase iron absorption
- Pair non-heme iron with a vitamin C source during the meal.
- Keep tea and coffee at least 60 minutes away from iron-rich meals.
- Separate calcium-rich foods or supplements from iron meals by about 2 hours.
- Prefer heme iron if you tolerate it, then layer in non-heme sources you handle well.
- Combine small portions of meat with lentils or beans to improve non-heme absorption.
- Use low FODMAP iron sources regularly if you are in a restriction phase, then re-expand.
- Time PPIs away from your highest-iron meal when possible, under clinician guidance.
- Aim for at least 7 hours of consistent sleep to support iron regulation and appetite.
- Avoid high-oxalate foods alongside your iron-focused meal when possible.
- If repletion is needed, prefer IV iron under medical supervision instead of routine oral trials.
- Use a liposomal oral iron only in very extreme cases when IV is not feasible, for the shortest time, and stop if IBS symptoms flare.
FAQ
What bowel conditions cause anemia?
Common GI causes include inflammatory bowel disease, celiac disease, peptic ulcer disease, colorectal cancer, angiodysplasia, and other sources of occult bleeding. Guidelines recommend evaluating iron deficiency anemia for gastrointestinal sources rather than assuming IBS alone.
Are IBS and anemia related
Yes. Systematic reviews describe lower baseline iron among IBS cohorts and clinical studies show that anemia in suspected IBS predicts organic disease rather than IBS itself. Major societies advise a structured GI evaluation when iron deficiency anemia is present. See the multicenter alarm-feature study and the IBS micronutrient review.
Next steps
Map your IBS subtype, correct the cause of low iron, and pick the least disruptive repletion path. If you want the full playbook built from over a thousand real cases, get the book IBSyncrasy and start personalizing your plan today. Buy the book.

Theodoros Prevedoros, MSc
The Microbiome Biochemist
With extensive experience evaluating over 3000 cases in various specialties, including gastroenterology, pediatrics, and endocrinology, Theodoros has collaborated with more than 25 doctors from Greece and Cyprus and over 10 laboratories worldwide.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
More posts