Post-infectious IBS treatment
Post-infectious IBS treatment should focus on reversing the biochemical and immune changes that the infection left behind and not only aim to calming pain and normalizing bowel habits. Care can be mainstream or personalized, but both work better when the barrier, immune tone, and neural signaling are considered together. Testing that profiles organisms and pathways helps target antimicrobials and microbiome supports while meal spacing and hydration improve engraftment.

Table of Contents
What is post-infectious IBS
and how does it relate to irritable bowel syndrome?
Post-infectious irritable bowel syndrome describes people who meet criteria for irritable bowel syndrome after an enteric infection such as infectious gastroenteritis, where symptoms persist even after the acute illness ends. In plain terms, a stomach bug can flip the gut into a sensitive mode that lingers. Large cohort reviews show the incidence of irritable bowel syndrome rises following infectious diarrhea, and the risk factors for development include severe initial illness, female sex, antibiotics during the infection, and baseline stress. Put simply, a tougher infection makes it more likely the gut stays reactive.
For quantification, risk of IBS is fourfold after infectious enteritis compared with uninfected controls, aligning with what many patients with IBS describe. Many people report a clear arc from infection to ongoing symptoms that matches postinfectious irritable bowel syndrome. In clinical notes, ‘post-infective irritable bowel’ is used when the infection link is clear, and the ‘syndrome’ label when symptoms persist for months
For quantification, risk of IBS is fourfold after infectious enteritis compared with uninfected controls, aligning with what many patients with IBS describe. Many people report a clear arc from infection to ongoing symptoms that matches postinfectious irritable bowel syndrome. In clinical notes, ‘post-infective irritable bowel’ is used when the infection link is clear, and the ‘syndrome’ label when symptoms persist for months
How to treat post infectious irritable bowel syndrome?
Treatment goals are to reduce gastrointestinal symptom burden, restore healthy bowel habit, and address the drivers left by the infection. Care generally starts with symptom-relieving options, then moves to pathway-matched plans informed by testing. This section covers both.
First-line options for treatment for post-infectious IBS
For people with diarrhea-predominant patterns, rifaximin reduces IBS-D symptoms in high-quality guidance, and short courses can be repeated if benefit wanes. In plain terms, a non-absorbed antibiotic can quiet overgrowth-like patterns without system-wide exposure. Probiotics can help selected ibs patients, but blends should be chosen by target such as gas, stool form, or pain rather than brand. Put simply, match the microbe to the job. Spacing meals protects fasting motility, and evidence shows that MMC occurs during fasting and feeding interrupts it, so many people notice less gas when the MMC runs.
Personalized testing in IBS patients and targeted care
Many do better with targeted diagnostics. PCR stool panels and shotgun metagenomics map organisms, while metatranscriptomics reveals active pathways like bile-acid genes or proteases that amplify symptoms in patients. In short, knowing who is present and what they are doing beats guessing. In pathway-matched care, botanicals or pharmaceuticals are selected for the organisms and mechanisms present, for example some respond to berberine derivatives while others to garlic organosulfurs, and yeast overgrowth requires antifungal planning. Personalization limits trial and error and can speed relief.
Why symptoms of post-infectious IBS persist?
Mechanisms you can address
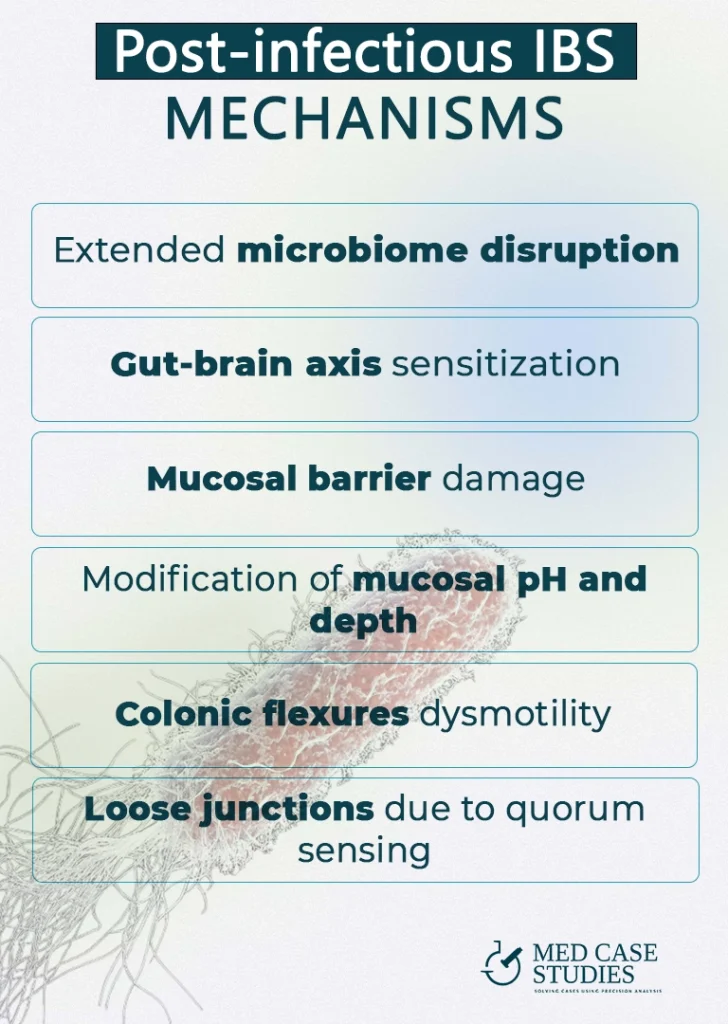
The after-effects of post-infectious illness touch several systems at once. Reviews of postinfectious ibs show that mechanisms include barrier dysfunction, immune activation, and sensory changes that heighten pain signaling. Importantly, there is huge difference between viral and bacterial post infectious development of irritable bowel syndrome. The lining gets leaky, nerves get jumpy, and microbes shift, and together they sustain symptoms. Let’s take a closer look:
Microbiome disruption after infectious gastroenteritis
An infectious hit can lower commensals and expand fermenters, raising gas and abdominal pain. The mix of bugs changes and produces more irritants. Toxins and enzymes from residual organisms can also stimulate secretion, which worsens stool form in post-infectious ibs.
Gut–brain axis sensitization in irritable bowel syndrome
After infection, colonic afferents become hyperexcitable and amplify normal distension, a hallmark of visceral hypersensitivity in IBS patients. The classic post-infectious neuronal data are shown in the Citrobacter rodentium DRG hyperexcitability paper, which maps well to urgency and pain.
Mucosal barrier and physicochemical shifts in post infectious states
Post-infectious states can thin mucus, alter pH, and reduce secretory IgA, which raises permeability. QS molecules can loosen junctions, and animal studies show that Pseudomonas increases intestinal permeability through interconnected quorum-sensing regulators. What this means for you, supporting the barrier can help many symptoms at once.
Motility changes and bowel habit at the colonic flexures
Infection-driven motility shifts can leave pockets of gas and stool at the splenic and hepatic flexures, which aggravates bowel habit variability. Traffic lights in the colon get out of sync. Spaced meals and morning activation with light hydration and movement help reset rhythms and reduce symptoms of ibs.
Microbe spotlights: Citrobacter, Pseudomonas aeruginosa, and Proteus mirabilis
-
Citrobacter with enterotoxin-driven secretion. Several infectious agent strains of Citrobacter freundii produce a heat stable enterotoxin identical to E. coli STa, which increases chloride secretion and fluid loss and this creates a path to lingering gastrointestinal symptom patterns. Evidence indicates that Citrobacter produces heat-stable toxin, and that secretion load can sustain loose stools.
-
Pseudomonas aeruginosa with quorum-sensing barrier effects. QS molecules such as 3 oxo C12 HSL modulate tight junctions and can raise permeability, and controlled models show that Pseudomonas increases intestinal permeability via interconnected regulators. Its chatter weakens the fence so irritants slip through.
-
Proteus mirabilis with mucin and IL 18 axis. Recent work suggests P. mirabilis lowers epithelial IL 18 which reduces mucin, and a thinner mucus layer heightens contact triggered abdominal pain. Supporting mucin and calming inflammation can ease reactivity, and one report shows that Proteus downregulates mucin production in inflamed tissue. Signals like these are also discussed in inflammatory bowel disease even when IBS is the main diagnosis.
learn how your gut works in real life and find your ibs type and treatment in IBSYNCRASY
-
DIAGNOSIS
TREATMENT
-
FOLLOW UP
How to treat post infectious irritable bowel syndrome?
Treatment works best when it is staged and personalized to your dominant mechanisms. PI-IBS includes diarrhea-predominant, constipation-predominant, and mixed patterns, and each pattern has different levers. Below is the plan I use with patients with IBS who describe an infection-linked onset.
Stage 1 Rhythm first: fasting, hydration, and a short low-FODMAP reset
- Fasting windows to engage the MMC. Eat your last meal before 20:00 and keep a 14-16 hour overnight fast to let the sweep return, as detailed in the MMC review. This improves bowel function and reduces gas trapping in the gastrointestinal tract.
- Hydration as “soil prep.” When you seed a probiotic or fiber, aim for stable daily fluids so engraftment is smoother in the gut mucus layer.
- Low-FODMAP for 2–6 weeks, then reintroduce. The controlled feeding trial by Halmos and colleagues showed fewer digestive symptoms during the structured phase, which simplifies later personalization.
Stage 2 Target the microbes implied by your tests
- Rifaximin for IBS-D phenotypes. Two-week courses reduced global symptoms, abdominal pain, and loose stool in the pivotal NEJM rifaximin trials, and rifaximin appears in the ACG pathway for treatment of IBS-D. This is classic treatment with antibiotics for a small bowel dysbiosis pattern.
- Individualized botanicals matched to ecology.
- When Proteus is detected, use allicin-rich garlic extracts as its urease biology permits.
- When swarming Enterobacterales dominate, use oregano oil constituents like carvacrol that reduce swarming and quorum activity, supported in in-vitro works.
- When Pseudomonas elastase signals are present, pair barrier-first care with temporary antigen lightening while you reduce burden, as shown in the elastase–gliadin study.
- Probiotics by function, not label. Choose strains that match your deficits rather than a generic mix. The best probiotic for postinfectious IBS is the one chosen from your omics map.
Stage 3 Repair the barrier and settle hypersensitivity
- Sodium butyrate support. Microencapsulated preparations have improved symptoms in IBS cohorts and support tight-junction integrity; see butyrate data.
- Bile-acid for IBS-D. If C4 or fecal bile acids are high, a sequestrant like colesevelam is effective in the phase 4 trial.
- Peppermint oil for cramping. Enteric-coated capsules rank well for pain and global symptoms, as summarized in the peppermint oil meta-analysis
Stage 4 Retrain the gut–brain axis
- Gut-directed hypnotherapy (GDH), in person or digital. Randomized data support GDH as part of integrated care; see the digital GDH RCT.
- Acupuncture or yoga as an add-on. Trials in diarrhea-predominant IBS and mixed phenotypes suggest improvements in pain and stool form. Examples include this acupuncture trial and a virtual yoga RCT
Stage 5 Precision additions and maintenance
- Antimicrobial cycles matched to targets. Short, pulsed protocols based on metagenomics for post-infectious IBS patterns, with re-testing to confirm changes.
- Food antigen management during barrier repair. When elastase or protease activity is high, lighten antigen load during therapy, then re-challenge.
- Re-inoculation and steady state. Once stable, maintain gains with targeted strains plus fiber blends. This is where IBS may shift into a durable remission for many.
FAQ
What is the best probiotic for postinfectious IBS?
Broad spectrum blends can help, but the best choice comes from testing such as PCR tests or shotgun metagenomics to identify organisms and pathways, then matching strains to gas, stool form, and pain targets
How common is post infectious IBS?
It is common after gastrointestinal infections and is a leading cause of new IBS. Meta analyses suggest a several fold increase compared with uninfected controls.
What causes post infectious IBS?
Most often bacterial infections, though viral and parasitic infections also contribute. Mechanisms include dysbiosis, barrier changes, immune activation, and neural sensitization.
How to treat post infectious irritable bowel syndrome?
Combine short course rifaximin in IBS D where appropriate, choose goal matched probiotics, protect fasting motility with meal spacing, and consider personalized diagnostics such as PCR, shotgun metagenomics, and metatranscriptomics to target organisms and pathways
Next steps
Ready for a precision workup? Book a 1:1 consult and we will align PCR, omics, and a targeted antimicrobial–microbiome plan to your gastrointestinal story.
Prefer a step-by-step guide first? My book IBSyncrasy includes a dedicated chapter on post-infectious IBS with exact timelines and dosing frameworks.
Want to read more cases? Start here: post-infectious IBS: viral vs bacterial and this digest on Pseudomonas spp high in stool.

Theodoros Prevedoros, MSc
The Microbiome Biochemist
With extensive experience evaluating over 3000 cases in various specialties, including gastroenterology, pediatrics, and endocrinology, Theodoros has collaborated with more than 25 doctors from Greece and Cyprus and over 10 laboratories worldwide.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
More posts