Creatine for autism
Is your child's brain starving?
Children with ASD often have lower creatine levels in certain brain regions which is critical for synapse maturation, brain energy and neuroplasticity.
💬 Did you know that creatine is the most important energy molecule during the first 2 years of life? Use the live chat in the bottom-right to ask me anything in real time.
Table of Contents
There are several different theories trying to explain the skyrocking increase in autism prevalence. But, autism is a syndrome. It is actually a spectrum of syndromes. Therefore it is impossible that there is a single etiology that can explain all the cases. And of course all the theories that have been proposed from time to time may explain only a few aspects of the autistic spectrum. Defects in creatine metabolism may explain different aspects in autism pathology and since creatine is a central energy molecule these defects have a place in almost all autism theories
Gene-Environment interactions in autism
One thing all theories agree on is that the manifestation of autistic behaviors and autism etiology stems from a combination of genetic and environmental factors. Indeed, there are hundreds of genes that have been studied in the context of autistic cases. However, in order for the specific genes to manifest their deleterious effects, they must be activated or aggravated by environmental factors. Of course there are also cases of chromosomal disorders that start at conception but they are only a small percentage as far as we know.
Gene | Environmental factor |
|---|---|
NLRP3 | Infection |
Arginase | Diet |
SHANK3 | Inflammation |
GAD | MSG |
Dopamine Receptor-1 | Screen time |
DPPIV | Dairy |
P450 | Toxic pollutants |
Energy harvesting from creatine
How does the brain decide what fuel will use?
A large part of the gene polymorphisms that have been documented for their relationship with the manifestation of autistic behaviors concern genes (and therefore proteins) which are related to the production of energy in the Central Nervous System.
“But most children on the spectrum do not have a lack of energy, on the contrary, hyperactivity is their main characteristic”
The above observation is logical, however the problem is not the amount of energy, but the distribution and above all the correct timing in providing it. Let me be clear.
The processes performed by our brain can be divided into two categories. In those that are done for the first time and in those that have been repeated so many times that they have become a habit. The unit of measurement of the difference between them can be defined as the experience. The more times an action or command is repeated, the “stronger” is the network of synapses and neurons that executes it. As a result, there are no energy leaks and the network performance is optimal; therefore, the energy required is minimal.
Take exercise for example. When someone does an exercise for the first time they usually fail and need much more energy to perform it. For this reason afterwards he is more tired and hurts more. But when he repeats it many times, the same exercise with the same weight becomes much easier, it is not tiring at all, and the energy required to do it correctly is only a small fraction of what was required the first time. The difference between them is the number of repetitions done, or experience. This applies to all our new “knowledge”. The first time it is something new, but after many times it becomes a habit.
Therefore, when we do something for the hundredth time, our body translates it as a habit and requires a small amount of energy for as long as we do it. In contrast, when we do something for the first time, very high amounts of energy are required in a very short time.
Energy
Experience
The more the experience the less energy required
What does autism have to do with it?
The fuel for first time learners is creatine
Let’s take tying shoelaces for example. Tying shoelaces is a process that seems extremely simple to an adult. The adult can perform it without even looking at his shoes, while he can very easily perform it while talking on the phone or watching TV. However, it is an extremely complex process that requires coordinated fine motor skills of both hands, eye coordination, timed movements and correct foot position. Dozens of muscles and nervous systems participate in this movement.
Now let’s see what happens when a child tries to tie his shoelaces for the first time. The vast majority of children will fail and it will take several dozen or hundreds of attempts to tie a rudimentary knot. So while the energy supply required by the adult for this process is minimal, the energy needs for the same process when a child performs it for the first time are enormous and for a short period of time. And the energy needs cannot be met by simple metabolic processes but a very rapid production of ATP is required for a short period of time.
This sharp and powerful burst of energy is what children need in order to learn everything and not just to tie their shoelaces. Speech, movement, associative thinking, sequential movements, the processing of commands, and all processes that require coordination of different synaptic networks are similar cases, which when performed for the first time (when learned) require large and rapid amounts of energy, while when repeated very often (experience) minimal amounts of energy are needed.
This extremely fast and short energy supply cannot be achieved through simple glucose metabolism or β-oxidation. So a different energy currency is needed. And that currency is phosphocreatine.
It is obvious that a newly developping brain, which has an enormous task load in order to fit in our information flooded society, needs a healthy and fully functional creatine energy system
Clear dosing ranges by age & body weight
Safety checklist (kidney labs, meds, who should avoid)
Progress tracker (speech, attention, motor learning)
Why is creatine better?
Quick energy in large amounts
Creatine is just an intermediate aminoacid. It is actually a carrier of the very important energy molecule ATP. Without ATP nothing really works in the body and during human evolution, all organs have adapted to use this highly efficient and ubiquitous molecule. After a relatively brief cascade of reactions located in the liver, the brain and the kidneys, substrates absorbed from our meals produce creatine, ATP is used to give energy to our nerve cells, and creatinine (the garbage created by this procedure) is excreted through our urine. This is a small journey for creatine considering the outmost importance it has and the consequenses of a dyregulated processing.
But, why we don’t we make ATP everytime we need it instead of storing it in the creatine form?
As discussed above, it’s all about speed. We know now that using our phosphocreatine reserve we can produce ATP almost 12 times faster than going the normal way of oxidative phosphorylation. Even more, this pathway is over 70 times quicker that making ATP from scratch. So phosphocreatine is like the accelarating switch when there is demand for quick and sophisticated thinking.
How is creatine made?
3 enzymes but dozens of accessory molecules
Creatine is synthesized in a two-step process in liver cells. The first step is a combination of two aminoacids, arginine and glycine. These aminoacids can be found in a wide range of foods, but in greater amounts in animal meat, like beef and chicken. Of course, you do not have to eat meat everyday in order to get the daily amounts of these aminoacids, since a well ballanced plant based diet can supply all the aminoacids we need. The enzyme responsible for this reaction is called arginine:glycine amidinotransferase (AGAT) and its action results in the production of ornithine and a very special molecule called guanidinoacetate (GAA).
The resulting GAA is then used to create creatine. This is accomplished with the help of a second enzyme called guanidinoacetate methyltransferase (GAMT). A critical cofactor in this process is another molecule called S-adenosylmethionine (SAMe). This step is the second checkpoint that is usually assessed when creatine deficiency is suspected. Also this is the point where most of the environmental insults may perturbate with the normal process, and most of the times in a reversible way.
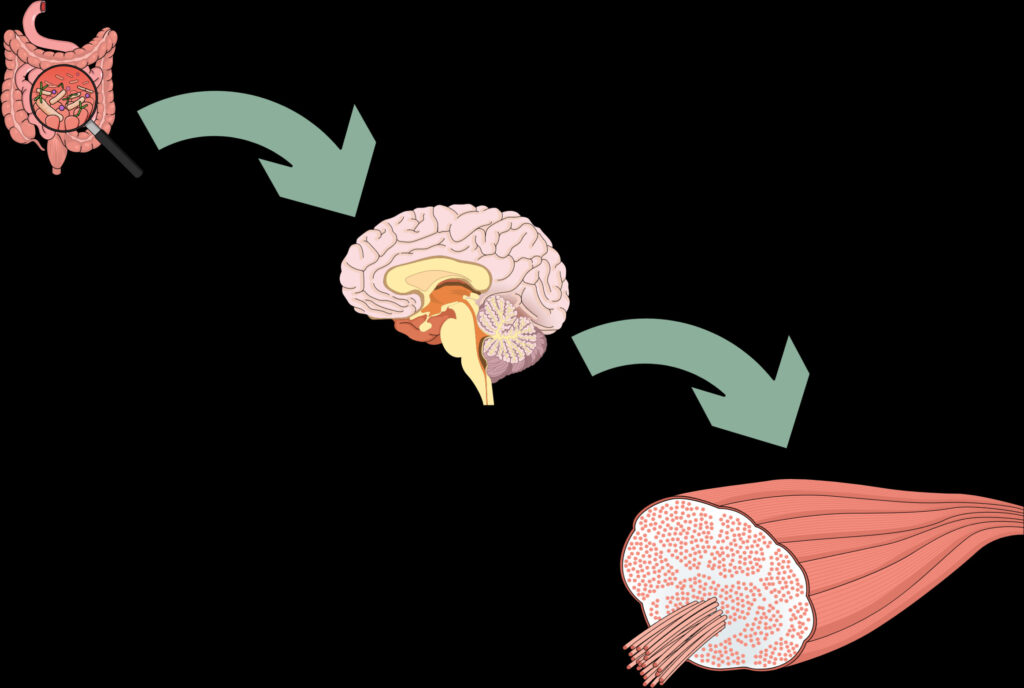
By now, creatine is ready to travel to the brain and muscle in order to store phosphate groups by forming phosphocreatine. This is the part where creatine needs to get into the corresponding tissues (brain, muscle). In order to gain access inside these tissues creatine needs to be transported via a transporter molecule. This molecule is expressed by a gene called SLC6A8, and is located on X chromosome. The fact that girls have two copies of this chromosome means that a mutation in one of the two copies may not lead to the disorder since they have the other copy intact and functional. On the other hand boys with this mutation are much more likely to exhibit creatine deficiency, because the only copy of the enzyme is defective and thus creatine cannot be used by the nerve cells.
STEP 1
AGAT enzyme combines aminoacids to produce the creatine precursor
STEP 2
The intermediate precursor is converted into creatine with the use of GAMT enzyme
STEP 3
The creatine molecule is transported inside the brain cells using SLC6A8
STEP 1
AGAT enzyme combines aminoacids to produce the creatine precursor
STEP 2
The intermediate precursor is converted into creatine with the use of GAMT enzyme
STEP 3
The creatine molecule is transported inside the brain cells using SLC6A8
Creatine deficiency - Beyond speech
Autistic children do not get the amount of instant energy needed for sustainable learning
As it is easily understood, any difficulty in providing energy from the creatine system and any deviation in the time it must be given leads to a very great difficulty in learning new things and performing new tasks.
No matter how many times a command (e.g., “Say the word water”) or the prompt for a movement (e.g., “Put the two puzzle pieces together”) is given, there must be an abundant supply of energy for the few seconds or fractions of a second that are required for its execution; otherwise, the command will fail. And the result of this lack of energy can be translated into our well-known symptoms of autism, such as dyspraxia, hypotonia, dysdiadochokinesia (touble executing consecutive functions), delay etc.
Hypotonia
By hypotonia we describe decreased muscle tone. Hypotonia should not be confused with muscle weakness or atrophy. Hypotonia is usually the result of a neurological problem. All the 3 enzymes described above, that take part in creatine biosynthesis and metabolism have been studied in hypotonic children.
Dyspraxia
Dyspraxia has an impact on the development of motor skills. Planning and performing fine motor activities are difficult for kids with dyspraxia. This can range from straightforward motor actions, like pointing, to more difficult ones (e.g., brushing teeth). Each child will experience dyspraxia differently in terms of severity and symptoms. Additionally, it may have varied effects on them at various phases of life. Dyspraxia, which is frequently divided into subcategories, can impair a wide range of fundamental daily activities. Again, creatine is a fundamental energy donor which should be timely activated in order to prevent fine motor activity impairements and dyspraxia.
Developmental delay
In males, clinical features range from mild to severe global developmental delay (GDD), intellectual disability (ID), seizures, behavioral and movement disorders. Clinical features in females range from asymptomatic to a severe phenotype similar to the phenotype in males.
Speech impairments
Speech is a process that needs high coordination involving multiple neurological systems. Creatine is the master molecule which provides the appropriate energy for speech development.
Deficiency continuum
Thousands of different phenotypes
Analyzing the literature one can notice that the cases of creatine deficiency that are commonly studied concern severe cases of autism. In addition, these cases are associated with a complete loss of functionality of one of the 3 main creatine metabolizing enzymes. These cases, however, represent one extreme in a wide range of phenotypes and for this reason it is believed that creatinopathies (cases of autism related to creatine metabolism) are less than 1% of the total number of autism diagnoses.
However, things are not exactly like that as there are additional cases in which the creatine system can be affected:
- Minor impact mutations affecting the 3 main genes
- Combination of mutations
- Alterations in accessory enzymes of creatine metabolism
- Deficiencies in cofactors and vitamins required for the correct usage of creatine
- Toxic effects that inhibit the otherwise normal function of creatine.
Therefore, there are not just two poles but a continuum of possible combinations of mutations and deficiencies that can lead to varying degrees of problem in creatine management. And since the creatine system is so prominent in the initial development of new skills and knowledge, even the slightest deviation can lead to symptoms. The following are some of the several hundred hypothetical cases along the continuum:
100%
Mild mutations or nutrient deficiencies
60%
Pathologic mutations giving symptoms
20%
Deactivated creatine system
A
Z
Fully functional creatine system
80%
Deleterious mutations in accessory enzymes
40%
Severely comprimizing creatine system defects
0%
Cautious treatment
Personalized dosage, custom diet, cautious monitoring
When the time for treatment comes, the easy thing to do is to give creatine to the child to see if some of his autistic traits improve. But this should never be done. The main reason is that creatine is the end product that the body needs. However, in order to be able to use it, co-factors, appropriate dosage, appropriate timing and above all attention to kidney function are required. For this reason the administration of high concentrations of creatine without proper supervision is something that should be avoided.
Incorrect side treatment
Even if the creatine dosage is correct, there several cofactors that should be administered simultaneously and within a specific time frame, in a personalized manner. Among them are magnesium, pyridoxale phosphate, S-adenosyl-methionine and other
Incorrect diet
To achieve maximum absorption but also to prevent interference from other elements consumed at the same time period, formulating an ideal diet is an important consideration when considering the usefulness of creatine. For example, certain carbohydrates interfere with the proper functioning of the creatine transporter.
Improper hydration
Whule it has not been verified by many studies, creatine seemt to increase the risk for kidney stones. For this reason, it is very important to monitor water intake of any child that takes creatine.
Incorrect creatine dosage
Creatine is an aminoacid. Like all aminoacids it needs specific transporters in order to be absorbed and properly utilized. In addition, it exhibits different absorption and reaction rates in relation to the conditions it is being used. This, the correct dosage is crucial to exploit creatine's full functionality
Not all mutations are treated with creatine
While creatine is the final product, several mutations affect its downstream utilization. In such cases, creatine is of no use and perhaps it may interfere with the absorption of other aminoacids
Treatment duration
Depending on the severity of the case and the age at which the intervention takes place, the time period in which the effect of creatine on the child's symptoms will be evaluated varies significantly. And for this reason, an intervention should not be considered failed unless it is given adequate time to act.
My experience
During my counseling years, my team has used various creatine regimens, both in boys and girls on the autism spectrum. In fact, many families had already tried a program that contained high doses of creatine. In some cases the program has had excellent results with the children’s parents and educators reporting significant progress within 2 to 3 months of starting the treatment. Many more cases reported gradual improvement in combination with other interventions. An additional feature is that in none of the cases was any side effect reported, nor worsening of symptoms. And this makes sense, since creatine is a completely natural substance that is used throughout the central nervous system as well as the musculoskeletal system.
Moreover, from my experience I know that even if the results of the creatine treatment are not so obvious, the improvement of the biochemical indices (creatine, creatinine, GAA, etc.) indicates that the metabolic pathways that rely on the appropriate use of creatine work better and more efficiently, which may prove to be very beneficial in the future.
Clear dosing ranges by age & body weight
Safety checklist (kidney labs, meds, who should avoid)
Progress tracker (speech, attention, motor learning)
Watch the video to understand why learning regression happens and the vast importance of creatine for proper brain connectivity
Takeaway message
It's about time to stop thinking of creatine as a bodybuilding supplement, but as an essential nutrient for normal brain development
References
Battini R, Leuzzi V, Carducci C et al. (2002). Creatine depletion in a new case with AGAT deficiency: clinical and genetic study in a large pedigree. Mol Genet Metab 77: 326–331.
Dhar SU, Scaglia F, Li FY et al. (2009). Expanded clinical and molecular spectrum of guanidinoacetate methyltransferase (GAMT) deficiency. Mol Genet Metab 96: 38–43.
van de Kamp JM, Betsalel OT, Mercimek-Mahmutoglu S, et al. Phenotype and genotype in 101 males with X-linked creatine transporter deficiency. J Med Genet. 2013;50:463–72.
Stöckler-Ipsiroglu, Sylvia, Olivier Braissant, and Andreas Schulze. “Disorders of creatine metabolism.” Physician’s Guide to the Diagnosis, Treatment, and Follow-Up of Inherited Metabolic Diseases. Springer, Cham, 2022. 235-249.

Theodoros Prevedoros, MSc
The Microbiome Biochemist
With extensive experience evaluating over 3000 cases in various specialties, including gastroenterology, pediatrics, and endocrinology, Theodoros has collaborated with more than 25 doctors from Greece and Cyprus and over 10 laboratories worldwide.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.
More posts