Depression and (eu)thyroid function
52 y.o female with depression and reduce functionality with normal TSH and T4 values

I hear a lot, from patients I consult that despite taking their thyroid medication for Hashimoto’s, they still experience thyroid symptoms. These symptoms usually are depressive thoughts, skin and hair problems, difficulty to focus, irritability, menstrual problems, chronic fatigue and many more. In other words, it seems that just by taking the active hormonal form is not sufficient for symptom reversal. Strange isn’t it? Well, if everybody knew the biochemical distance between orally taking a drug and its final destination, it wouldn’t seem so strange. In addition, blood tests are indicative of the adequacy of a substance, and not necessarily of it’s efficiency. Some of the stages a drug needs to pass before exerting it’s beneficial actions are:
- Intestinal absorption
- Liver inactivation
- Target organ reach
- Tissue distribution
- Cellular uptake
- Carrier-molecule adequacy
- Receptor ligation
In fact, the line between drug taking and drug efficiency may be defined by just a small mutation in any of the proteins participating in the thyroid drug cascade. Just like in Mary’s case.
Mary C. was a 52 years old housewife, mother of 3 boys. She gave birth to her last son when she was 41. 3 years later he was diagnosed with mild mental retardation. Mary was diagnosed with Hashimoto’s hypothyroidism 6 years ago. At first she started experiencing fatigue with no apparent reason. A few months later depressive thoughts appeared. She’s on levothyroxine (75 mg) ever since and her endocrinologist insists that her thyroid function is well adjusted. The only clue he had, though, was Mary’s serum TSH and T4 values.
Mary visited her first psychiatrist at the age of 47, and has since visited 3 more. All of them prescribed psychiatric treatment, and in all cases, the treatment helped for a few months and then stopped. All these treatments included at least one drug from the family of SSRI’s. Their action permits serotonin to act longer on the system, and in this way they reduce depressive thoughts. Mary was desperate so she turned to controversial treatments. Again, she did not find any help. When I got her detailed history I could not find a very important element that could lead me to a diagnostic plan. The only thing I was able to appreciate a little more is the fact that her young son is mentally retarded. And I guess it was enough.
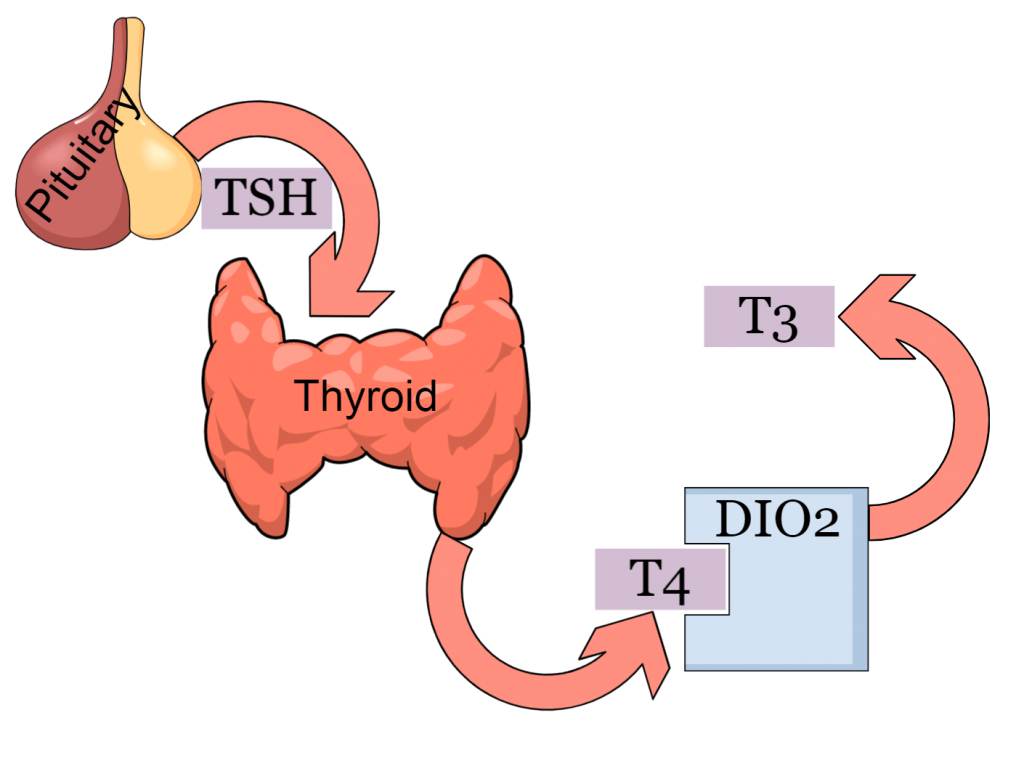
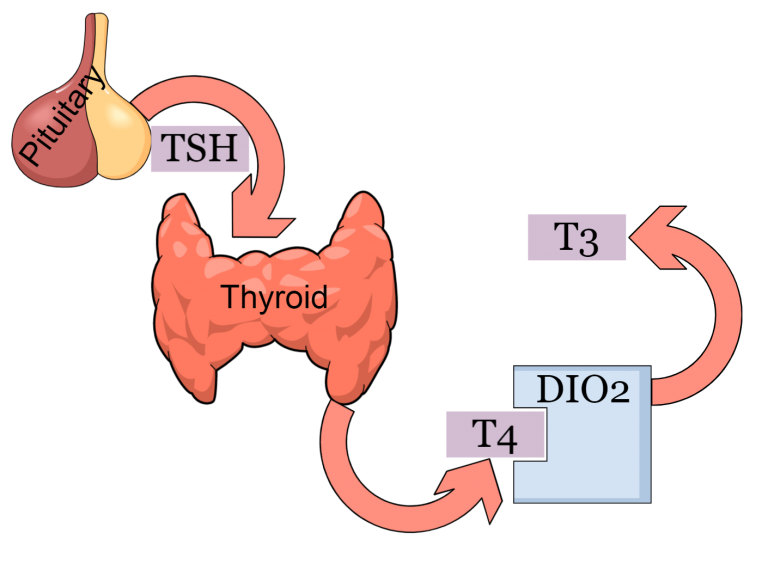
The production of the active T3 molecule requires several steps. First, the pituitary gland, located in our brain, produces the Thyroid Stimulating Hormone. Next, TSH will travel down to the thyroid gland and inform it that the T4 molecule has to be released. T4 is the inactive pro-hormone containing 4 atoms of iodine. Then, another enzyme takes turn, called DIO2 (Deiodinase-2), which is responsible for the removal of an iodine atom and the production of the final active hormone, namely T3. Finally, T3 is ligated to its respective receptors throughout the whole body and exerts its beneficial actions.
There are several polymorphisms (different forms) which make the DIO2 enzyme less productive. Under certain circumstances, when more T3 is needed, the enzyme cannon meet the demands. One of these polymorphisms, perhaps the most studied one is rs225014. It is estimated that about 12% of the total population possesses this polymorphism in an homozygous manner (both from the father and the mother). This polymorphism produces lower local T3 values (local means skeletal muscle and pituitary) but normal serum values. In addition, it is studied in the context of mental retardation. In short, I asked Mary to perform a WGS (Whole Genome Sequencing) and several biochemical and vitamin indices. Also, a urine reverse T3, although of low diagnostic value, could exclude hormone inactivation.
Mary’s DNA uncovered an homozygous polymorphism (rs225014). This variation is reported to be associated both with impaired baseline psychological well-being and enhanced response to combination T4/T3 therapy. This effect is achieved without affecting serum thyroid levels. It has also been reported that this polymorphism favors the development of a mental retardation phenotype, especially in iodine-poor regions.
DIO2 (rs225014)
Downregulation of T3 production in selected areas of the body
Vitamin D3 deficiency
Vitamin D3 deficiency has been linked to increased frequency of depressive behaviors
Panicker, Vijay, et al. “Common variation in the DIO2 gene predicts baseline psychological well-being and response to combination thyroxine plus triiodothyronine therapy in hypothyroid patients.” The Journal of Clinical Endocrinology & Metabolism 94.5 (2009): 1623-1629.
Guo, T. W., et al. “Positive association of the DIO2 (deiodinase type 2) gene with mental retardation in the iodine-deficient areas of China.” Journal of medical genetics 41.8 (2004): 585-590.
According to the literature, there are two ways to improve DIO2 function. The first one is a natural flavonoid called kaempferol, commonly found in apples, grapes, onions, brocolli, several berries and other plants. Kaempferol is shown to increase DIO2 activity by a factor of 10. The second option is treatment with both T4 and T3 in combination, using an empiric analogy. After talking to her endocrinologist and explaining the situation, Mary agreed to proceed with both options. Mary reported an impressive benefit form the combinational therapy, and until today she is on it.
Da-Silva, Wagner S., et al. “The small polyphenolic molecule kaempferol increases cellular energy expenditure and thyroid hormone activation.” Diabetes 56.3 (2007): 767-776.
Bianco, Antonio C., and Elizabeth A. McAninch. “The role of thyroid hormone and brown adipose tissue in energy homoeostasis.” The lancet diabetes & endocrinology 1.3 (2013): 250-258.
The only reason Mary kept coming is to adjust her dosage and perform preventive tests and treatments. This case highlights the need for personalized treatment, since small modifications of an already taken treatment may result in tremendous improvements.
- Normal serum T4 and T3 values do not represent the levels existing locally in some organs
- About 10 percent of the population carries an homozygous polymorphism on the DIO2 gene, which is responsible for the conversion of T4 to T3
- Combination T4 + T3 therapy should be considered after testing for the gene polymorphism
- In the absence of any mutation, kaempferol is an excellent alternative option which may increase DIO2 activity up to 10 times
- Post traumatic stress events have the possibility to epigenetically alter the activity of several enzymes, including DIO2

With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.