Case study of PPIs causing irritable bowel syndrome (IBS)

Number of cases
Mean age
Rate of success
Treatment duration
Most common symptom
Most common culprit
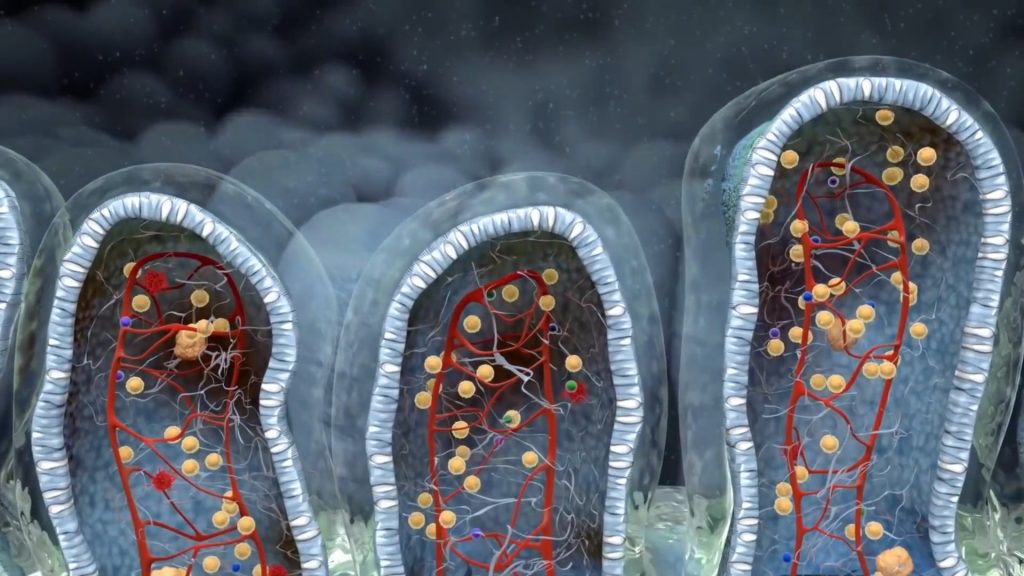
Gastric acid is a major component that delineates the delicate balance between successful digestion and malabsorption, playing a critical role in conditions such as irritable bowel syndrome and reflux disease. In addition, our gut lumen is primarily an acidic environment due to the presence of stomach acid, and it should be treated as such. Any interference, such as drug administration (including over-the-counter medications), hormonal imbalance, or environmental input, disrupts the timely and adequate production of hydrochloric acid, leading to malabsorption and gradual alteration of intestinal physiology. The most common symptoms triggered by chronic PPI use are small intestinal bacterial overgrowth, flatulence, altered stool habits, and gas, which are often associated with heartburn.
Regrettably, the number of patients remaining on PPI treatment for more than 24 weeks is steadily increasing, primarily due to the rapid and efficient symptomatic relief it provides for conditions like heartburn and reflux disease. Often, physicians themselves recommend that the patient continues the treatment, although there are cases where patients persist with the treatment despite their physicians advising them otherwise. Moreover, most patients continue the treatment even after being diagnosed with B12 deficiency. Oral bacteria such as Fusobacterium, Porphyromonas, Tannerella, and others capitalize on the more hospitable gastric environment and may infiltrate the gut and circulation, predisposing individuals to various other disorders, including cardiovascular, metabolic, autoimmune diseases, and even cancer.
George was a typical case of unnecessary chronic PPI use. His symptoms started very mild. He was prescribed omeprazole for just a 2-day incident of gastric reflux. The relief was immediate and with the consent of his doctor, George was still on PPI’s 6 years later!!
His lifestyle pattern set the stage for his stomach symptoms. Many coffees, very late dinners, no salads, and symptoms that kept changing and worsening. Episodic, diarrhea, unexplained fatigue… Several years later, he was still on the stomach treatment but his life was a mess. He had already consulted several specialties and performed tests like gastroscopy and colonoscopy without significant findings, except non-specific gastritis and redness throughout his colon.
The stomach is the first part of the digestive tract that suffers from the consequences of a long-term poor diet and bad habits
Chronic PPI use gradually lessens the production of stomach acid, thereby permitting oral bacteria and indigested food to enter the lower GI system
Hypochlorrhydria and hypergastrinemia, both consequences of chronic acid suppression lead to vitamin inadequacies and hormone dysfunction
IBS is an inevitable effect of chronic acid suppression and it may take several forms (constipation, bloating, diarrhea, etc.)
Aware of the harmful effects PPIs, such as omeprazole, have on the GI system and the hormonal changes that occur following their chronic administration (e.g., gastrinemia), I asked George to undergo several stool and blood tests. I wanted to rule out some of the most severe side effects of chronic acid suppression, like hypochlorhydria, exocrine pancreatic insufficiency, and ADMA (an early indicator of hypertension). Additionally, I aimed to assess the extent of microflora distortion and the degree of SIBO to plan appropriate treatment, considering the symptoms of IBS, such as abdominal pain and digestive issues.
The quality and the quantity of indisgested particles that reach the colon are the determining factors of fermentation rate (and gas production)
Chronic lowering of acid production makes the stomach less capable of digestion. And while acid-induced pain is limited, dyspepsia is heightened.
The trapped air within the colon along with the loss of defecation timing leads to the constant feeling of colonic content and bowel movement
Besides B12 deficiency, which is the commonest culprit of chronic acid suppression, many more vitamins and nutrients are depletes through indirect consequences of hypochlorhydria
In cases like this, certain tests, including the hydrogen breath test, consistently return positive results. The small intestinal microbiome may comprise only a small portion of the total bacterial load of the GI system, but it can take advantage of the persistent low gastric acid (hypochlorhydria) and expand manyfold, leading to acid reflux and other symptoms. Several more results should be evaluated collectively before proposing a treatment plan to address the small intestinal bacterial overgrowth and related symptoms.
Low diversity index
Fragments and residues of indigested food particles produce mixed movements of the gut giving rise to alternating defecation pattern
Elevated ADMA
Dysregulated nitric oxide metabolism leads to fluctuation in blood pressure. Elevated ADMA is detected in chronic PPI users
SIBO
Bacterial overgrowth of the small intestine interferes with proper absorption of nutrients and produces gas
Probiotic sterility
Probiotic sterility leads to abnormal fermentation of starch, sugars, and fiber. Bloating and gas are the main symptoms
In George’s case (and all similar cases) the treatment plan should cover the entire gastrointestinal system. Gastric inflammation reduction, small intestinal overgrowth reduction, and colonic microbiome restoration. Although it is a very difficult and possibly time-consuming process, there is no other way to complete healing. Many factors also play a major role: Patient’s age, gallbladder removal, diet, and of course lifestyle habits. The rule is “the earlier the intervention, the better the results”.
Our third appointment was done by phone because he was out of the city. He told me that although he had seen a significant improvement in his stool pattern -one or two times per day, nearly formed- he had also noticed an increase in his allergic symptoms. I explained to him that this was normal and something desirable. As the histamine-producing bacteria die off they release histamine in large quantities. I also explained that this exacerbation of his allergies would be greatly reduced when he completed both antimicrobial treatments. He had managed to eat mostly before 9:00 pm and to take his breakfast after 10 am. Although this was a great accomplishment I urged him to take his dinner even earlier than that…
Long-term PPI use causes a multitude of changes in both the secretory machinery of the digestive tract and the gut microbiome. The secretion of hormones like gastrin, acetylcholine, and histamine is compromised and the continuous enrichment of the small intestine with oral and environmental bacteria inevitably leads to small intestinal bacterial overgrowth. This is why IBS is much more prevalent in past or current users of this kind of medication. PPis, like omeprazole, are not designed to be taken for more than 8 consecutive weeks.
- Long-term PPI use, such as omeprazole, disrupts gastric acid production and intestinal physiology, leading to IBS symptoms like small intestinal bacterial overgrowth, flatulence, and altered stool habits
- Chronic acid suppression from PPIs can result in hypochlorhydria, vitamin deficiencies, and hormone dysfunction, ultimately causing IBS symptoms like bloating and gastric discomfort
- Tests confirm small intestinal bacterial overgrowth, low diversity index, elevated ADMA, and probiotic sterility, which are associated with PPI-induced IBS
- Treating PPI-related IBS symptoms requires a comprehensive approach that targets gastric inflammation, small intestinal overgrowth, and restoration of the colonic microbiome, with early intervention yielding better results
- IBS is more prevalent in past or current users of PPIs like omeprazole, which are not intended for use beyond 8 consecutive weeks, due to the medication's effects on secretory machinery and gut microbiome

With a background in Chemistry and Biochemistry from the National and Kapodistrian University of Athens, Theodoros brings a wealth of knowledge in functional medicine and advanced treatments to his role. He possesses exceptional skills in analysis, pattern recognition, diagnostic translation, and storytelling. He is also FMU certified in Functional Medicine and has received training in advanced treatments from the Saisei Mirai Clinic in Japan.